Measurements in diagnosis of craniocervical dissociation:
Basion-Dens Interval (BCI):
>12 on radiographs
>8.5 on CT
Powers Ratio > 1.0
Atantodental Interval
>3 in Adults
>5 in Children
Atlanto-occipital Interval
>2 in Adults
>5 in Children
Atlanto-axial Interval
>3.5 in Adults
>4 in Children
Basion-dens interval and Power Ratio
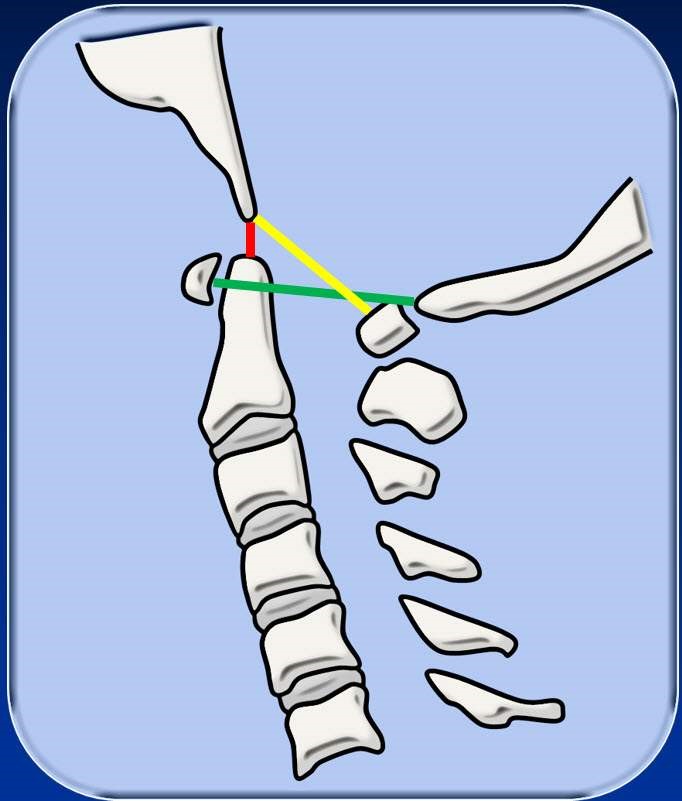
The basion-dens interval is the distance between the tip of the clivus and dens (red line). A basion-dens distance of >12 mm on radiographs and >8.5 mm on CT is suggestive of craniocervical instability.
The Powers ratio is the ratio of the distance between the basion and the posterior spinolaminar line of C1 (yellow line) and the distance between the opisthion and the anterior arch of C1 (green line). A ratio (yellow line/green line) of greater than 1.0 is suggestive of craniocervical instability.
Atlantodental joint or interval
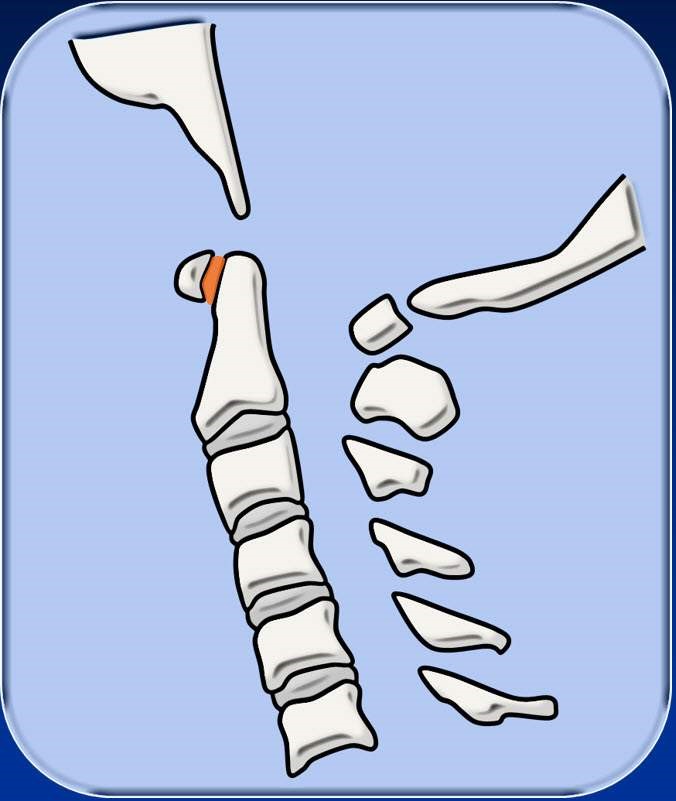
The atlantodental joint or interval is the space between the anterior arch of C1 and the dens (orange). Widening of the joint can be used to detect instability at the C1-C2 level. Pathologic widening of this space is considered greater than 3 mm in an adult and 6 mm in a skeletally immature patient.
Atlanto-occipital and atlanto-axial joints.

Typically there is close, symmetric apposition of the atlanto-occipital (orange) and atlanto-axial (yellow) joints.
For the atlanto-occipital joint, an absolute distance of >2 mm in adults and >5 mm in children is suggestive of craniocervical injury.
For the atlanto-axial joint, an absolute distance of >3.5 mm in adults and >4 mm in children is suggestive of craniocervical injury.
There is significant variability in the normal atlanto-occipital and atlanto-axial distances. Therefore, asymmetric widening of the joint by >1-2 mm should also be suspicious for ligament injury.